Chapter 7 Respiratory acid-base disorders
7.1 Classification of respiratory acid-base disorders
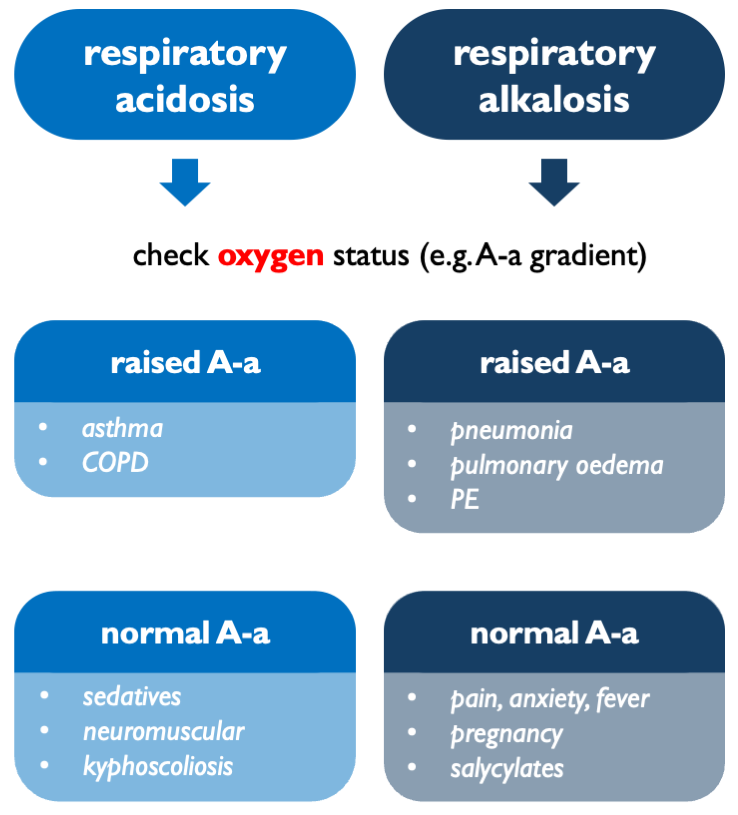
The main step in classifying respiratory acid-base disorders is to work out whether they are arising in the lung or centrally (i.e. neural control of breathing). Formally, that can be assessed by checking the A-a gradient. In practice, that is usually determined by clinical gestalt: e.g. is the SaO2 appropriate for the FiO2?
In respiratory acidosis:
- high A-a gradient = impaired gas transfer (V/Q mismatch, diffusion impairment, shunt…)
- normal A-a gradient = pure hypoventilation (CNS depression, obesity, neuromuscular…)
In respiratory alkalosis:
- high A-a gradient = hypoxia-driven hyperventilation (PE, pneumonia…)
- normal A-a gradient = central hyperventilation (anxiety, salicylates…)
7.2 A-a gradient
The A-a gradient is the difference between the partial pressure of O2 in the alveloi, PAO2 (calculated) and in arterial blood, PaO2 (measured).
\[\begin{equation} \text{A-a gradient}=PAO_2-PaO_2 \tag{7.1} \end{equation}\]
7.2.1 Alveolar gas equation
PAO2 is calculated using the alveolar gas equation:
\[\begin{equation} PAO_2=FiO_2(P_{atm}-P_{H_2O})-\frac{PaCO_2}{R} \tag{7.2} \end{equation}\]
For patients breathing room air at sea level and on a balanced diet, this can be approximated as:
\[\begin{equation} PAO_2 (\text{in kPa}) \approx 20-\frac{PaCO_2}{0.8} \tag{7.3} \end{equation}\]
assuming:
- FiO\(_2\) \(\approx\) 0.21
- P\(_{atm}\) \(\approx\) 101 kPa
- P\(_{H_2O}\) \(\approx\) 6.3 kPa
- R \(\approx\) 0.8
…and to convert from kPa to mmHg, multiply by 7.5
7.2.2 Explanation
The partial pressure of oxygen in the alveoli will be determined by the maximum available O2 (FiO2 \(\times\) P\(_{atm}\)) minus ‘space’ occupied by water vapour (as per Dalton’s law or partial pressures) and minus O2 consumed by metabolism.
So, \(PAO_2 = \text{inspired } O_2 - O_2 \text{ lost to metabolism}\).
Metabolic O2 consumption is inferred from CO2 production, i.e. PaCO2. CO2 production is less than O2 consumption. This discrepancy is described by the respiratory quotient, \(R = \frac{\dot{V}CO_2}{\dot{V}O_2}\). Typically, R ~ 0.8, meaning that for every 10 O2 molecules consumed, 8 CO2 molecules are produced. Therefore, \(O_2 \text{ lost to metabolism} \approx \frac{PaCO_2}{R}\).
R varies with metabolic fuel:
- CHO: R = 1.0
- fat: R = 0.7
- protein: R \(\approx\) 0.8
So:
- most patients on a mixed diet, R \(\approx\) 0.8
- fasting / ketotic, R closer to 0.7
- getting TPN on ITU, R closer to 1.0
7.2.3 Interpretation
\[\begin{equation} \text{A-a expected (kPa)} \approx \frac{\text{age}}{30}+0.5 \tag{7.4} \end{equation}\]
So normal A-a gradient is very approximately:
- 1-2 kPa in young adults
- 2-3 kPa in middle age
- 3 kPa in elderly
Interpretation is best validated for patients on room air. Once on supplemental O2, the gradient becomes larger and is harder to interpret.