Chapter 17 Calcium
17.1 Ca2+ homeostasis
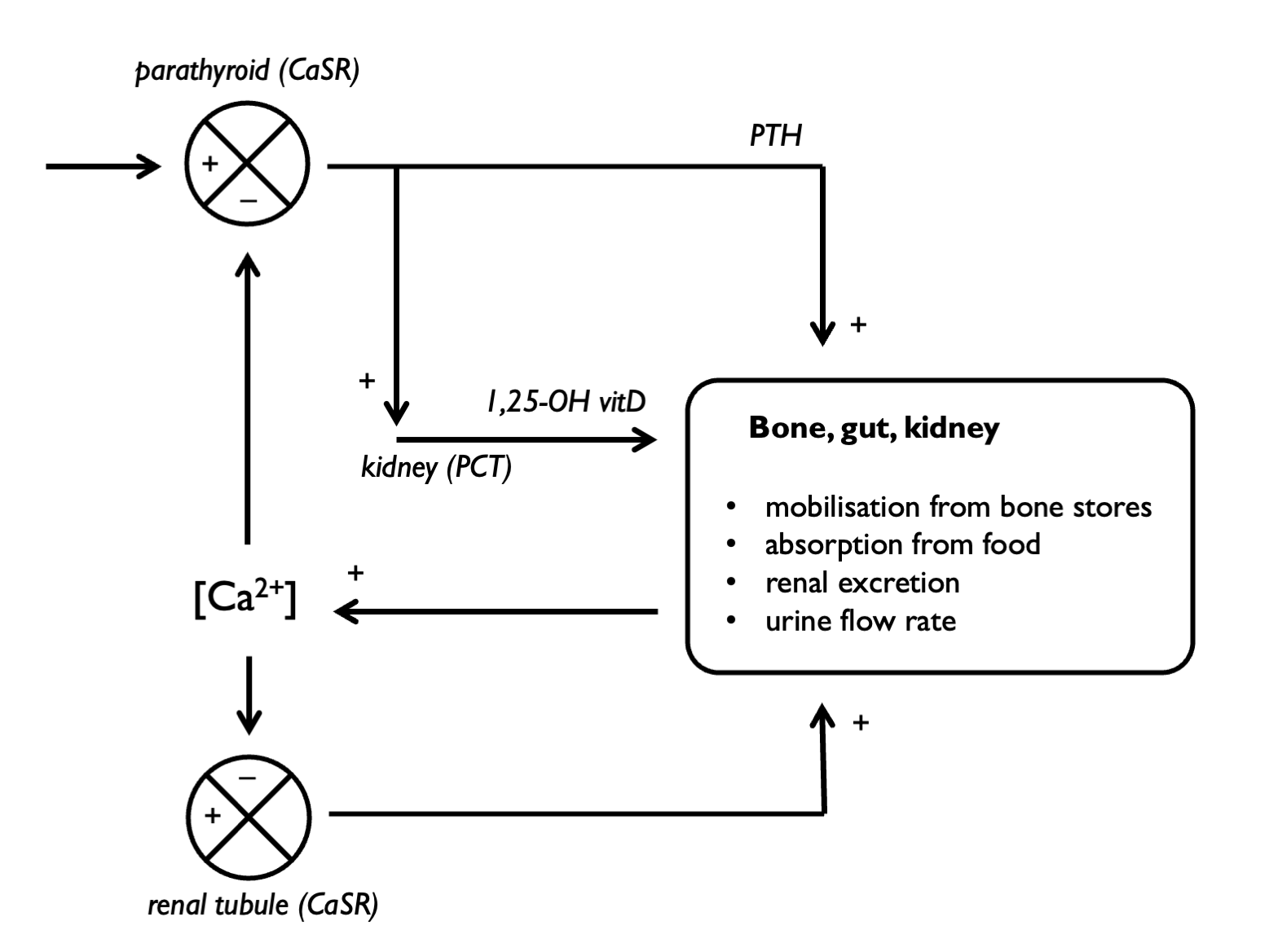
Serum calcium is regulated by PTH and vitamin D:
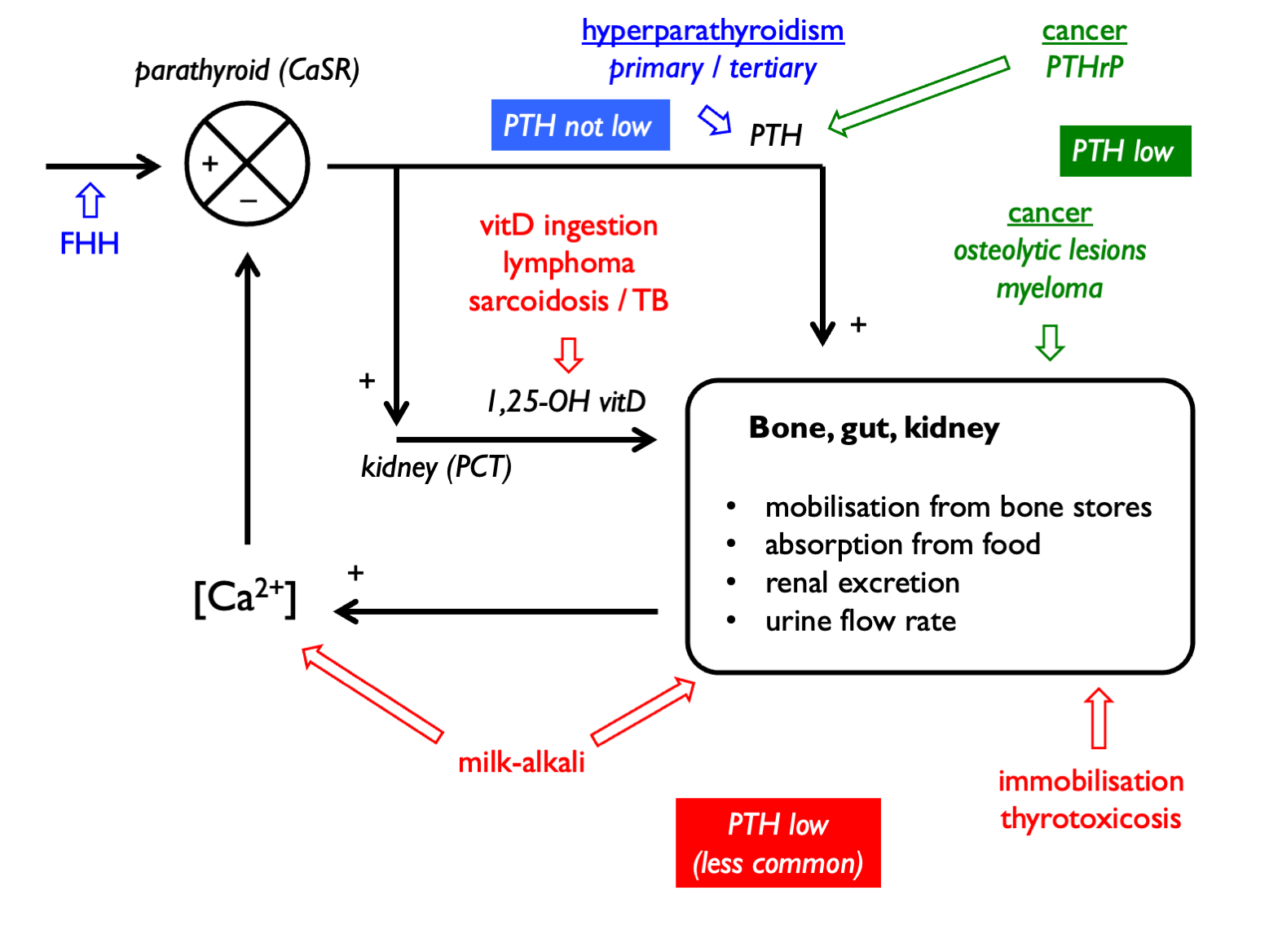
Hypercalcaemia can be classified as PTH-dependent or PTH-independent:
17.1.1 Drug causes of hypercalcaemia:
| Mechanism | Drugs |
| Impaired urinary Ca2+ excretion | thiazide diuretics |
| calcium-containing antacid preps (calcium-alkali) | |
| lithium | |
| Increased absorption | vitamin D preparations |
| calcium-containing antacid preps (calcium-alkali) | |
| Stimulation of PTH secretion | lithium |
| Reduced bone buffering | vitamin A |
| anti-oestrogens |
17.1.2 Polyuria in hyperCa
Activation of the basolateral CaSR in TALH stimulates NKCC2, inducing a NaCl diuresis. Activation of the apical CaSR in collecting duct inhibits AQP2, inducing a NDI. These responses have presumably evolved as a defence against kidney stones, but in the context of pathological hypercalcaemia result in polyuria. Therefore management of hyperCa involves copious NaCl (e.g. aiming for u/o 100 - 150 ml/hr). The rationale is to replace NaCl losses and also to encourage calciuresis by driving Na-coupled calcium excretion in PCT.
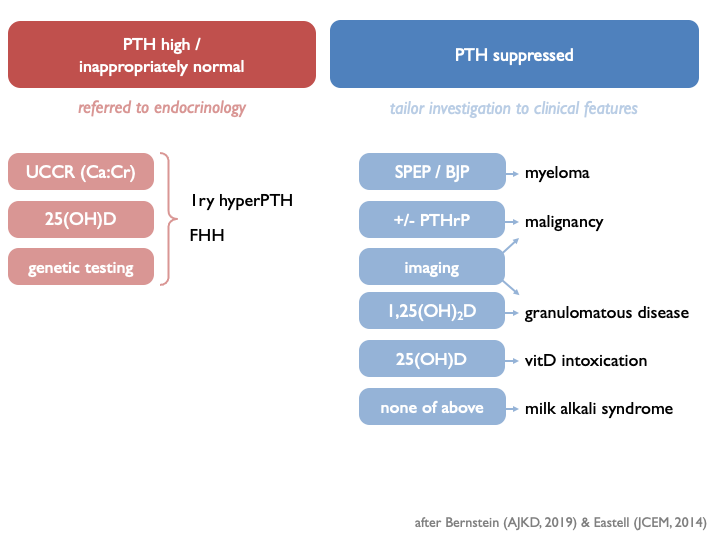
17.2 Investigations in hypercalcaemia:
 See alkalosis chapter for a description of the calcium-alkali syndrome.
See alkalosis chapter for a description of the calcium-alkali syndrome.
17.3 Urine calcium
Urine calcium excretion will vary according to calcium intake and urinary sodium excretion (with UCa and UNa changing in parallel) (Foley & Boccuzzi, 2010). There is also diurnal variation.
Therefore urine calcium excretion is best assessed on 24 hr collection, rather than spot samples.
Results may be expressed either as:
- total calcium excretion (as mg per kg BW per day)
- 24hr calcium-creatinine clearance ratio, CCCR
- calcium / creatinine excretion ratio (as mg/mg or mmol/mmol)
(The CCCR is often referred to as the FECa, but given the extent to which serum calcium is protein-bound, it may not be appropriate to think of it as such.)
CCCR performs best as a screening test for familial hypocalciuric hypocalcaemia (Christensen et al., 2008).
Random spot urine samples may be used (but are less accurate) and are normally interpreted as:
- calcium / creatinine ratio (mg/mg or mmol/mmol)
17.4 Interpreting the results
17.4.1 Unit conversions
Ca: 1 mg = 0.025 mmol Cr: 1 mg = 0.0088 mmol
Therefore, a Ca/Cr of x mg/mg = 2.84x mmmol/mmol.
17.4.3 Hypercalciuria (e.g. in hyperPTH, other causes of hypercalcaemia, RTA):
- >4 mg per kg per day
- >300 mg (= 7.50 mmol) per day (men) or >250 mg (= 6.25 mmol) per day (women)
- Ca/Cr ratio > 0.6 mmol/mmol = 0.20 mg/mg (adults) - or > 0.15 mg/mg in second void urine after an overnight fast
- FECa > 2 % (CCCR > 0.020)
In an observational study of stone-formers (Curhan, KI 2001), stone risk elevated at thresholds lower than these classical cut-offs of 300 mg (M) or 250 mg (F) - but stone risk obviously complex and related to other urinary salts / pH etc.
Two implications of hypercalciuria are:
- risk of stones / nephrocalcinosis
- risk of bone demineralisation
17.4.4 Hypocalciuria (e.g. FHH, Gitelman):
- FECa < 1 % (CCCR < 0.010)
In a small Japanese cohort of adult patients with Gitelman syndrome, calcium excretion was ~ 10-fold lower than in matched controls (Cheng et al., 2007):
- 24hr excretion ~20 vs ~200 mg
- FECa ~0.15% vs ~1.5%
- Ca/Cr ~0.006 vs ~0.06 mg/mg (= ~0.02 vs ~0.2 mmol/mmol)