Chapter 15 Hyperkalaemia
15.1 Causes of hyperkalaemia
- spurious
- distribution (ECF/ICF shifts)
- impaired renal K+ excretion
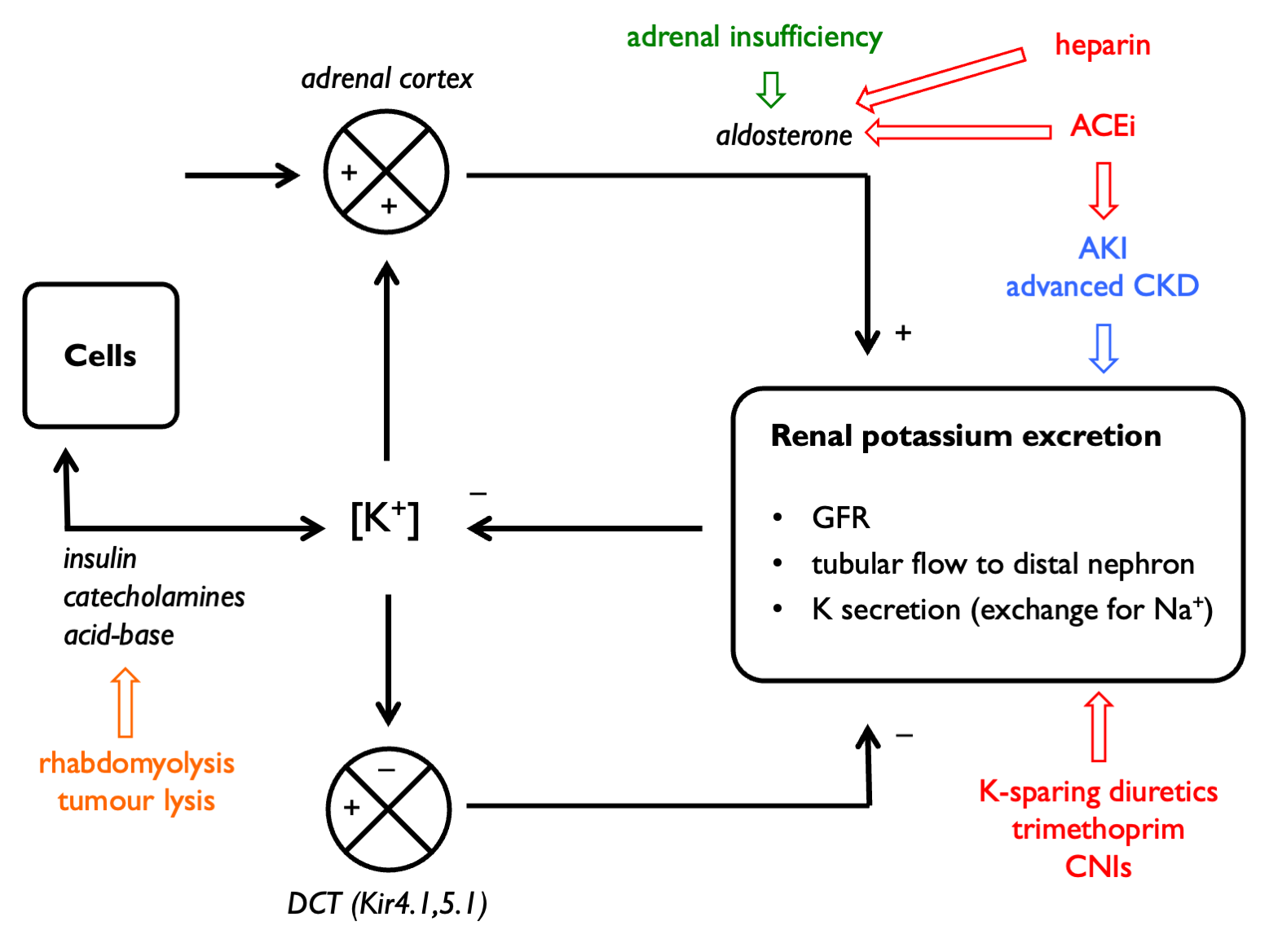
Renal excretion of K+ may be impaired if any of the following are limited (Hunter & Bailey, 2019):
- GFR
- tubular flow rate
- delivery of Na+ to the distal nephron
- aldosterone signalling in the distal nephron
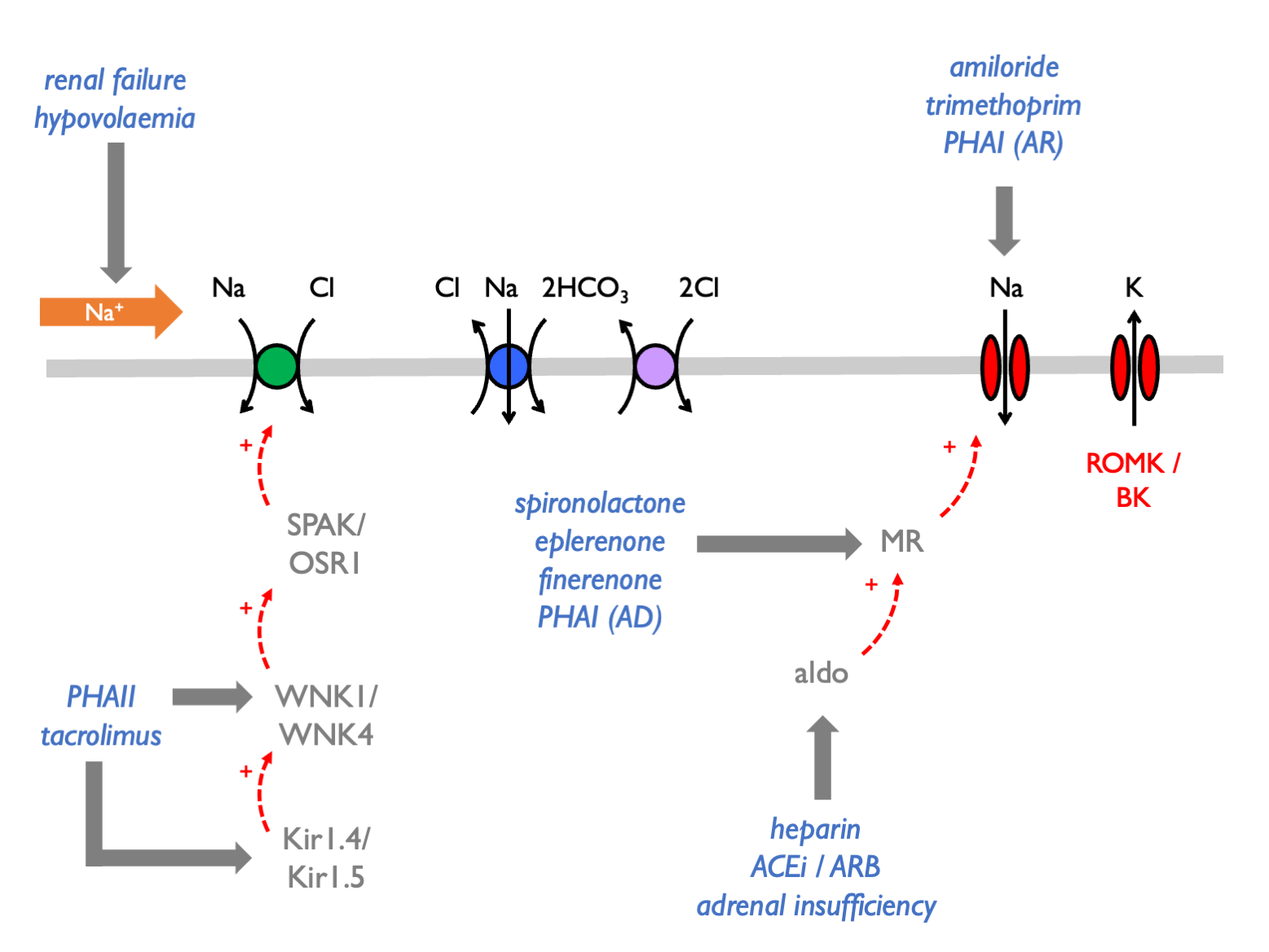
 Hyperkalaemia is often due to an inappropriate shift from electrogenic to electroneutral Na+ reabsorption:
Hyperkalaemia is often due to an inappropriate shift from electrogenic to electroneutral Na+ reabsorption:
Therefore the causes of hyperkalaemia are:
| EXCESSIVE K LOAD | diet | high-K diet |
| drugs | IV penicillin | |
| TRANSCELLULAR SHIFTS | cell injury | rhabdomyolysis |
| beta-blockers | ||
| digoxin | ||
| anaesthetic agents | ||
| mannitol | ||
| RENAL IMPAIRMENT | renal impairment | AKI / CKD |
| DEFECTIVE ALDOSTERONE SIGNALLING | impaired renin secretion | DM |
| beta-blockers | ||
| NSAIDS | ||
| ACEi | ||
| ARBs | ||
| Addison’s | ||
| heparins | ||
| ketoconazole | ||
| PHAI | ||
| spironolactone / eplerenone | ||
| DEFECTIVE ELECTROGENIC NA TRANSPORT | ENaC blockade | PHAI |
| amiloride / triamterine | ||
| trimethoprim | ||
| pentamidine | ||
| lithium | ||
| PHAII | ||
| CNIs |
Use FECl response to thiazides as functional test for PHAII (normal response is < 3% increment).
15.2 Causes of spurious hyper- and hypokalaemia
PseudohyperK from K-EDTA contamination.
PseudohyperK due to prolonged delay prior to centrifugation (blood cells leak K in cold weather).
PseudohypoK due to prolonged delay prior to centrifugation (blood cells take up K via Na-K-ATPase in the warm; “seasonal pseudohypoK” in summer).
PseudohyperK due to leucocytosis (WBC > 70) – K released from cells during clot formation (test by measuring serum and plasma K simultaneously).
Familial hyperK due to abnormalities in RBC membrane permeability.