Chapter 4 Acid-base & chloride
4.1 Acid-base homeostasis
Summary of the dietary sources of acids and alkali and the role of the kidney in generating bicarbonate (to aid the excretion of non-volatile acid):
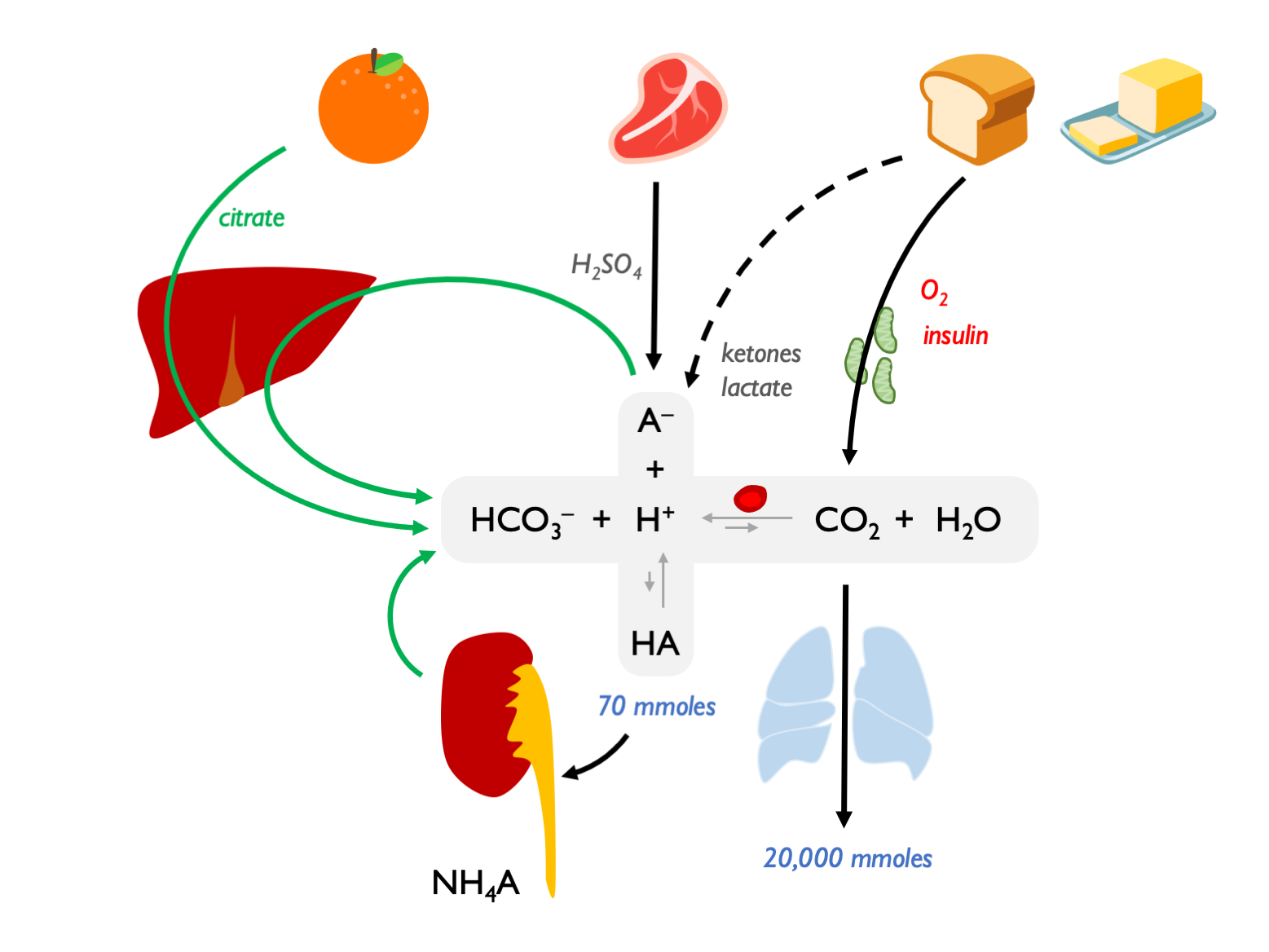 In the tissues, CO\(_2\) diffuses into RBC and converted to HCO\(_3\); HCO\(_3\) then exported on AE1 (band 3) = chloride / Hamburger shift. In the lungs, HCO\(_3\) re-imported into RBCs (so chloride shifted back out again), converted to CO\(_2\) and exhaled; transport direction reverses as CO\(_2\) gradients reverse. This process is important for enhancing the efficiency of CO\(_2\) transport – means that the majority of circulating CO\(_2\) can be in the form of HCO\(_3\).
In the tissues, CO\(_2\) diffuses into RBC and converted to HCO\(_3\); HCO\(_3\) then exported on AE1 (band 3) = chloride / Hamburger shift. In the lungs, HCO\(_3\) re-imported into RBCs (so chloride shifted back out again), converted to CO\(_2\) and exhaled; transport direction reverses as CO\(_2\) gradients reverse. This process is important for enhancing the efficiency of CO\(_2\) transport – means that the majority of circulating CO\(_2\) can be in the form of HCO\(_3\).
(And as RBCs take up CO\(_2\) and acidify, O\(_2\)-Hb dissociation curve shifts to the right, aiding O\(_2\) tissue delivery: Bohr effect.)
4.2 pH
\[\begin{equation} pH=-log[H^{+}] \tag{4.1} \end{equation}\]
\[\begin{equation} H^{+} = 10^{pH} \tag{4.2} \end{equation}\]4.3 Carbonic acid buffer system
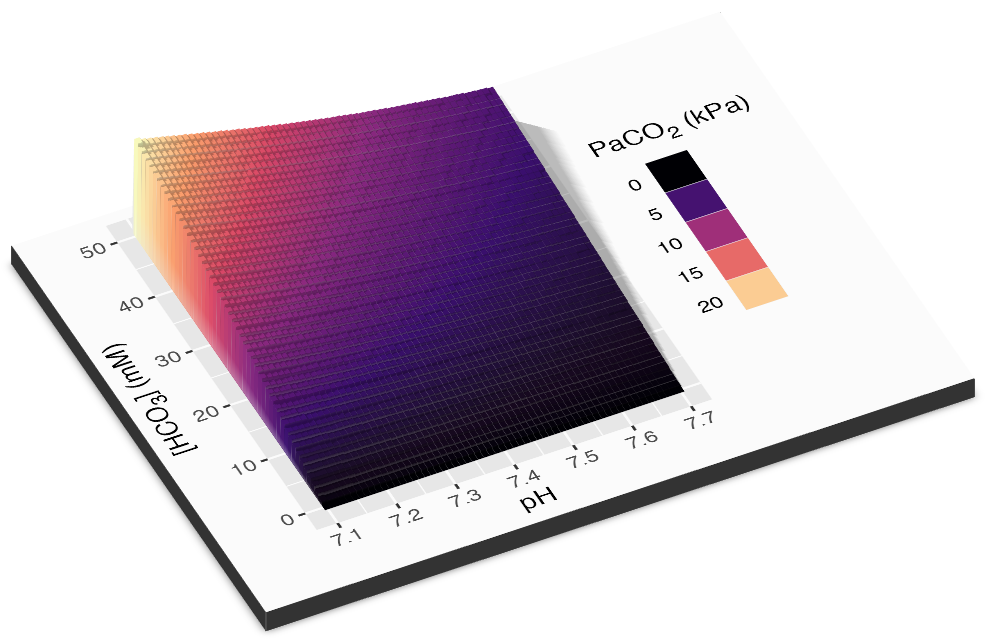
The relationship between pH, PaCO2 and HCO3 is described by the Henderson-Hasselbalch equation:
\[\begin{equation} pH = pKa+log \frac{[A^-]}{[HA]} \tag{4.3} \end{equation}\]
\[\begin{equation} pH = 6.1 + log \frac{[HCO_3]}{\alpha .PaCO_2} \tag{4.4} \end{equation}\]
This relationship can be visualised in 3D…
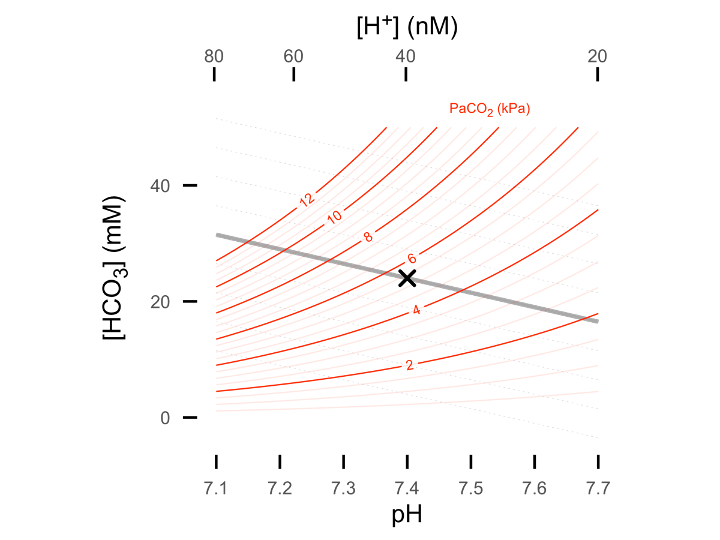
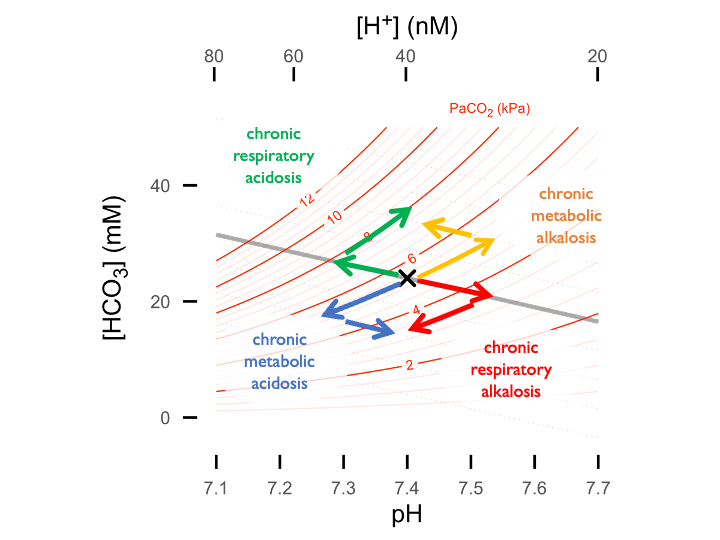
…or 2D in the form of a Davenport plot (shown below) - or alternatively as a Siggard-Andersen plot (pH vs. PaCO2 with BE nomogram lines). See interactive plotting app.
4.4 Renal control of acid-base homeostasis
Renal net acid excretion is determined by urinary titratable acid, ammonium and bicarbonate:
\[\begin{equation} NAE = V \times (U_{NH_{4}^+} + U_{TA} - U_{HCO_{3}^-}) \tag{4.5} \end{equation}\]
In the face of a daily acid load, the main job of the kidneys is to regenerate HCO3 for the ECF in order to replace that lost through buffering of non-volatile acids. It does this through mechanisms that keep urine pH ~ 6 to minimise risks of uric acid precipitation (in acid urine) or calcium phosphate precipitation (alkaline urine).
The three key processes are:
- reabsorption of filtered HCO3
- excretion of titratable acid (H2PO4) = net HCO3 reabsorption
- excretion of ammonium (glutamine > NH3 + H+ > NH4+) = net HCO3 reabsorption
4.4.1 Normal renal response to chronic acidosis
The normal response of the kidneys to chronic acidosis is to upregulate urinary NH4 excretion. This was illustrated in historical acid-loading studies:
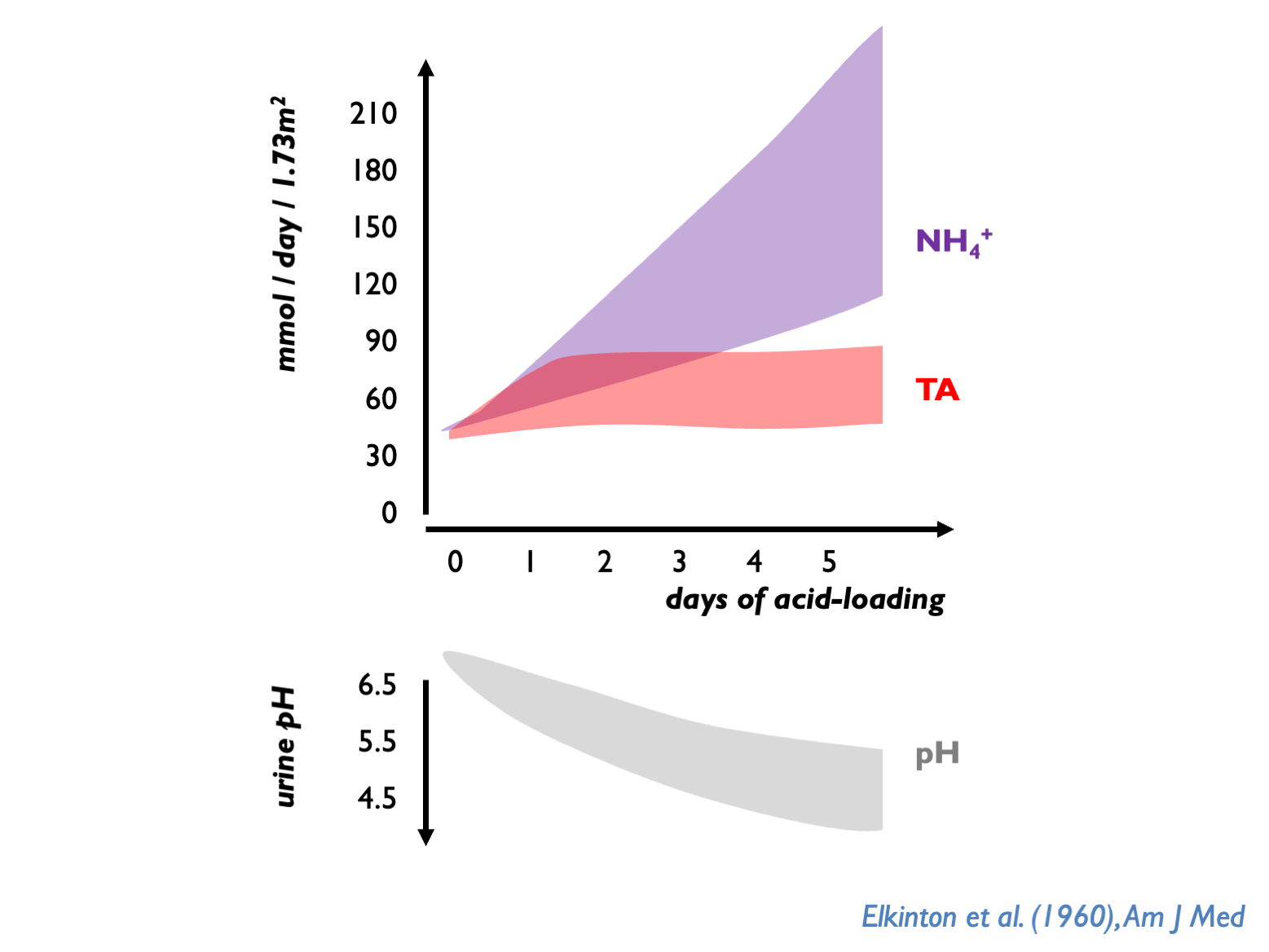
The preferential use of NH4 over TA is probably an evolutionary defense against kidney stones. NH4 tends to keep upH around 6.0 - thus avoiding very acid urine (risk of uric acid precipitation) or very alkaline urine (risk ofCaHPO4 precipitation).
Normally, kidney has to dispose ot 70 mmol non-volatile acid per day through TA and NH4. uNH4 therefore normally 30 – 40 mmol per day; up to 100 - 200 mmol per day after acid-loading (Kamel & Halperin, KI Reports 2021; Uribarri, AJKD 2022). uNH4 (directly-measured) higher on Western than plant-based diets (Uribarri AJKD 2022).
4.4.2 Citrate metabolism in acidosis
In reponse to chronic acidosis, the proximal tubules also increase citrate reabsorption (with consequent hypocituria).
Hypocituria is a common risk factor for urolithiasis. (See also this chapter and review.)
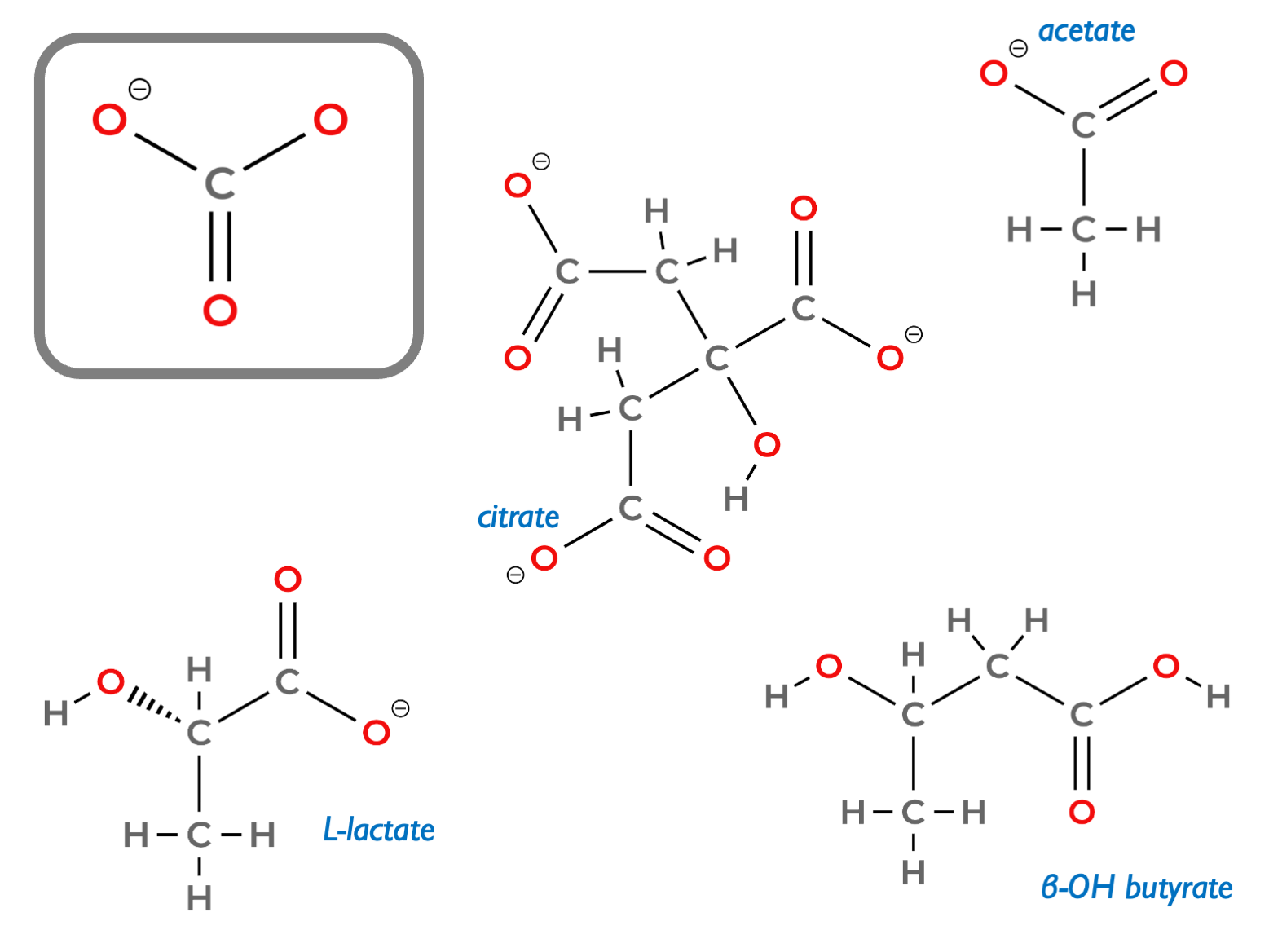
Citrate is present in diet: high in citrus fruits and coconut water. Is filtered by glomeruli and reabsorbed in the PCT by the sodium-dicarboxylic acid cotransporter, NaDC1. (Citric acid is of course a tricarboxylic acid.) Metabolised in rpTEC mitochondria in citric acid cycle to make CO2 and H2O, generating bicarbonate (3 molecules HCO3 per 1 molecule of citrate). Analagous to citrate metabolism in the liver and muscle. The 1:3 stoichiometry should be obvious looking at the molecular structure of citrate (shown below with other bicarbonate precursors, that have 1:1 stoichiometry):
Blood citrate concentration low (~100 mcM) but still makes contribution to systemic acid-base homeostasis as ~10 – 30 mmol filtered and ~6 – 24 mmol reabsorbed daily, so approximating 20 – 70 mmol HCO3 equivalent.
NaDC1 is upregulated in response to metabolic acidosis: presumably evolved as a defence against systemic acidosis by retaining alkali.
Citrate is the most abundant urinary organic base and the most important chelator for urinary calcium. Therefore hypocituria causes calcium oxalate / calcium phosphate stones.
Risk factors for hypocituria:
- dietary (high meat / high Na / low fruit)
- dRTA (due to systemic acidosis / hypoK)…
- …but not Fanconi pRTA (as cannot reabsorb filtered citrate)
- chronic diarrhoea (due to metabolic acidosis / hypoK)
- chronic GI malabsorption / Roux-en-Y bypass
- hypokalaemia (see below)
- topiramate (due to metabolic acidosis)
- thiazides (due to hypoK)
The effect of hypoK causing hypocituria explained as hypoK causing intercellular acidification of rpTECs, so stimulating the Na-citrate co-transporter.
Treatment of hypocituria:
Can measure 24 hr citrate excretion or just treat empirically in most stone-formers:
- dietary measures
- K citrate supplements
K citrate has been shown to reduce urinary calcium excretion in CaOx stone-formers (perhaps due to correction of acidosis / correction of hypoK / binding calcium in the gut).
4.4.3 Renal response to alkalosis
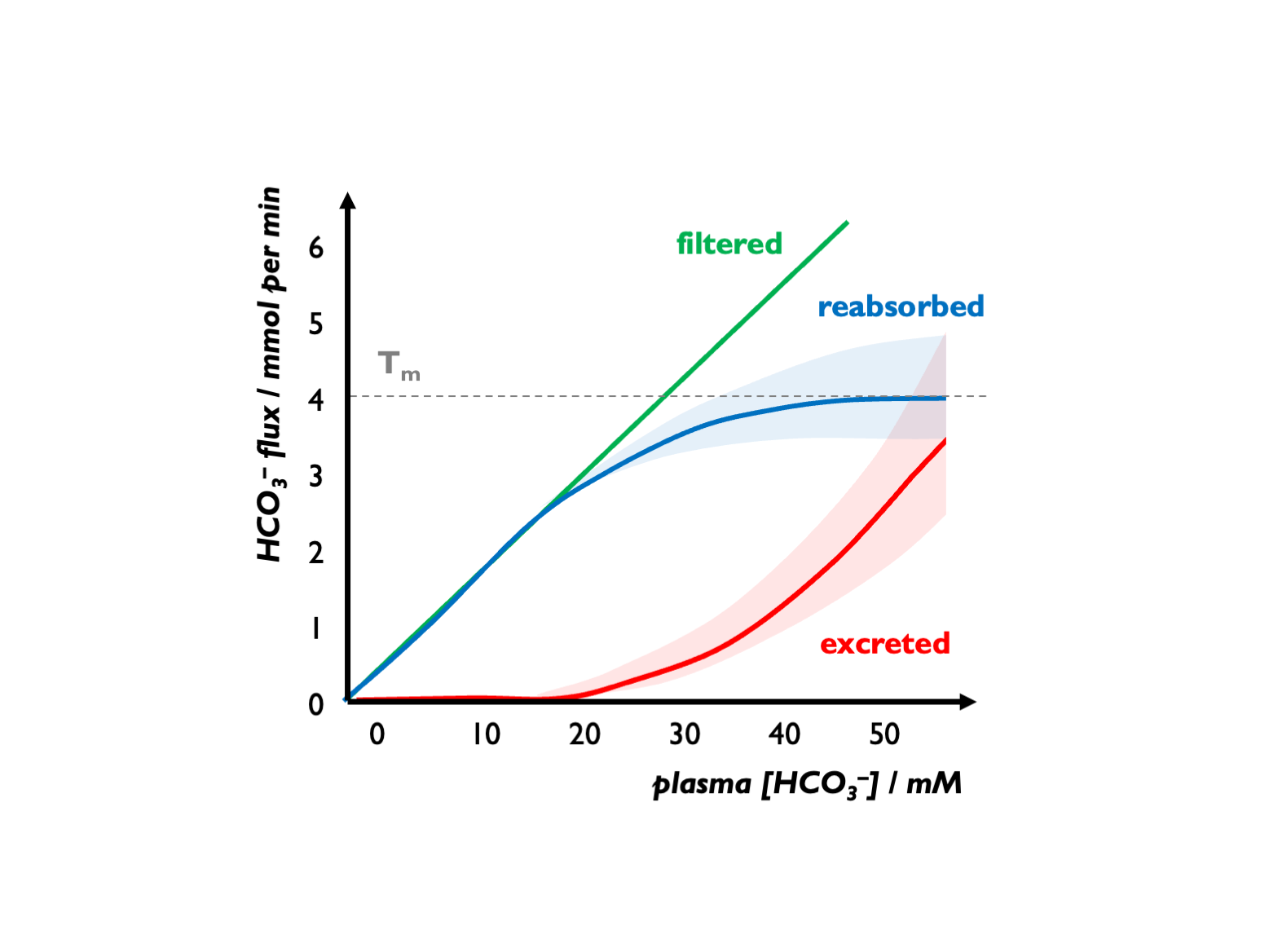
An alkalosis will correct automatically as HCO3- exceeds the Tm.
There is an apparent Tm for HCO3-, set close to 25 mM but variable and influenced by various factors (GFR, luminal pH, hormonal factors etc.) For example, during volume depletion, stimulation of Na reabsorption (NHE activity) will increase HCO3- re-absorption, so leading to an increase in the apparent Tm for HCO3-. Under normal circumstances, FEHCO3 is < 0.1% (Lote).
In alkalosis, bicarbonaturia can drive cation loss (e.g. hypokalaemia)